Janda Philosophy
Janda’s approach to the evaluation and management of chronic musculoskeletal pain focuses on the importance of the central nervous system in mediating chronic pain through neuromuscular imbalance.
Structure vs. Function
In musculoskeletal medicine, there are two main schools of thought, that is, a structural or functional approach. In the structural approach, the pathology of specific static structures is emphasized; this is the typical orthopaedic approach that emphasizes diagnosis based on localized evaluation and special tests (X-Ray, MRI, CT Scan, etc). On the other hand, the functional approach recognizes the function of all processes and systems within the body, rather than focusing on a single site of pathology. While the structural approach is necessary and valuable for acute injury or exacerbation, the functional approach is preferable when addressing chronic musculoskeletal pain.
The Sensorimotor System
In chronic pain, special diagnostic tests of localized areas (for example, low back radiographs) are often normal, although the patient complains of pain. The site of pain is often not the cause of the pain. Recent evidence by supports the fact that chronic pain is centrally-mediated (Staud et al. 2001). Similarly, research on the efficacy of different modes of exercise management of chronic pain has shown a central effect of exercise in decreasing chronic low back pain (Mannion et al. 1999). This research supports the basis of Janda’s approach: the interdependence of the musculoskeletal and central nervous system. Janda states that these two anatomical systems cannot be separated functionally. Therefore, the term “sensorimotor” system is used to define the functional system of human movement. In addition, changes within one part of the system will be reflected by compensations or adaptations elsewhere within the system because of the body’s attempt at homeostasis (Panjabi, 1992).
The muscular system often reflects the status of the sensorimotor system, as it receives information from both the musculoskeletal and central nervous systems. Changes in tone within the muscle are the first responses to nociception by the sensorimotor system. This has been supported by various studies demonstrating the effect of joint pathology on muscle tone. For example, the presence of knee effusion causes reflex inhibition of the vastus medialis (Stokes & Young, 1984). The multifidus has been shown to atrophy in patients with chronic low back pain (Hides et al. 1994), and muscles demonstrate increased latency after ankle sprains (Konradsen & Raven, 1990) and ACL tears (Ihara & Nakayama, 1986). The global effect of joint pathology on the sensorimotor system was demonstrated by Bullock-Saxton (1994). She noted a delay in firing patterns of the hip muscles and decreased vibratory sensation in patients with ankle sprains.
Because of the involvement of the CNS in muscle imbalance and pain, Janda emphasizes the importance of the afferent proprioceptive system. A reflex loop from the joint capsular mechanoreceptors and the muscles surrounding the joint is responsible for reflexive joint stabilization (Guanche et al. 1995; Tsuda et al. 2001). In chronic instability, deafferentation (the loss of proper afferent information from a joint) is often responsible for poor joint stabilization (Freeman et al. 1965).
Tonic and Phasic Muscle Systems
Janda identified two groups of muscles based on their phylogenetic development (Janda, 1987). Functionally, muscles can be classified as “tonic” or “phasic”. The tonic system consists of the “flexors”, and is phylogenetically older and dominant. These muscles are involved in repetitive or rhythmic activity (Umphred, 2001), and are activated in flexor synergies. The phasic system consists of the “extensors”, and emerges shortly after birth. These muscles work eccentrically against the force of gravity and emerge in extensor synergies (Umphred, 2001).
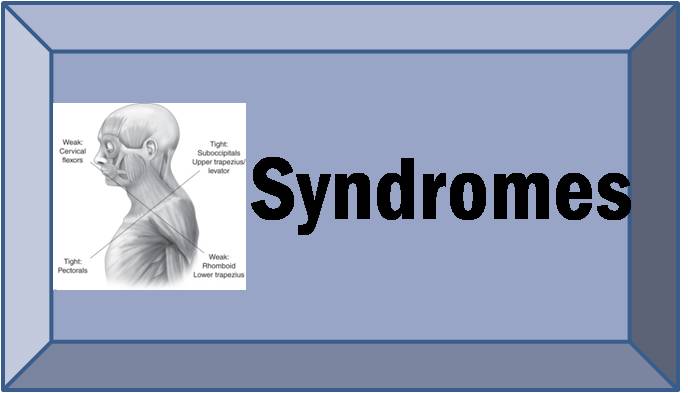
Janda noted that the tonic system muscles are prone to tightness or shortness, and the phasic system muscles are prone to weakness or inhibition (Table 1). Based on his clinical observations of orthopedic and neurological patients, Janda found that this response is based on the neurological response of nociception in the muscular system. For example, following structural lesions in the central nervous systems (such cerebral palsy or cerebrovascular accident), the tonic flexor muscles tend to be spastic and the phasic extensor muscles tend to be flaccid. Therefore, patterns of muscle imbalance may be due to CNS influence, rather than structural changes within the muscle itself.
It’s important to note that this classification is not rigid, in that some muscles may exhibit both tonic and phasic characteristics. It should also be noted that in addition to neurological predisposition to tightness or weakness, structural changes within the muscle also contribute to muscle imbalance. However, in chronic pain that is centralized within the CNS, patterns of muscle imbalance are often a result of neurological influence rather than structural changes.
| Tonic Muscles
Prone to Tightness or Shortness |
Phasic MusclesProne to Weakness or Inhibition |
| Gastroc-SoleusTibialis Posterior
Hip Adductors Hamstrings Rectus Femoris Iliopsoas Tensor Fascia Lata Piriformis Thoraco-lumbar extensors Quadratus Lumborum Pectoralis Major Upper Trapezius Levator Scapulae Scalenes Sternocleidomastoid Upper limb flexors |
Peroneus Longus, BrevisTibialis Anterior
Vastus Medialis, Lateralis Gluteus Maximus, Medius, Minimus Rectus Abdominus Serratus Anterior Rhomboids Lower Trapezius Deep neck flexors Upper limb extensors |
Table 1: Tonic & Phasic Muscles